 |

|
|
|
|
 Back to 1996 2nd Quarter Table of Contents
Back to 1996 2nd Quarter Table of Contents
Exponential growth is the unique charac-teristic of life. Destruction of a cancer colony by x-ray therapy follows unique exponential form. The primary target of x-rays (ioniz-ing electromagnetic radiation) must be that reaction which is responsible for exponential growth. Because exponential growth is inher-itedthischemicalreactionmustbethecreation of life, of cancer and this target. 434 MHz UltraHighFrequencynon-ionizingradiation increasesthex-raykillperunitdosewhilsten-hancing its exponential character. Both must target the same chemical system of glutathione becauseincyclicconversionsofreduced →oxi-dized →reduced forms, energy is produced exponentially. This cycle has been named Re. The additional energy for this cyclic reaction Re is supplied by the anaerobic glycolysis of one molecule of d-glucose converting to two molecules of l-lactic acid. MethodsData was accumulated from cancer patients treated under seven different regimes.
Conventional X-irradiation.
7. UHF irradiation after intravenous injections of cysteine and GSSG administration. 1. 31 Outram Street West Perth 6005 Western Australia ResultsThestandardequationrelatingcellkill in-vivo in a human cancer colony is: NR = NO (1-(1-e-D Where NR represents the number of cells remainingafterNOareradiatedwithadaily dose of D rads for a total of y days. e is the baseoftheexponentiallogarithm,DOisthat dose which is required to kill 37% (1/e) of the colony at a single dose and x is the number of targets in each cell which must be killed by the x-rays to kill the cell. This equation can be derived at simply.1 1. Conventional X-irradiationApplying this relationship to conventional normothermic in-air radiotherapy a minimum value of x = 2 can be established. Whenxexceeds5,cureofthiscancerwithin the limit of tolerance of the human body cannotbeachievedbyteletherapyalone.1,2,3 Because the cyclic transformations between reduced (GSH) and oxidised (GSSG) produce energy (electrons) in exponential quantities with time and x-rays kill (thus reducing energy production) by a directly opposing function (and UHF increases this exponential kill) therefore the target x is identical to Re, or the glutathione cycle, which may be active or inactive in each cancer cell’s cytosol, as shown in Figure 1 (page101). The radiosensitivity value, DO , iscalculatedtobeapproximately160to180 rads under normothermic in air radiation. 2. X-irradiation under three atmospheres absolute pressure hyperbaric oxygenationHead and neck cancer and some skin cancers arising from the female genitourinary tract are tolerant of X-ray therapy under three atmospheres of absolute pressure of oxygen. Six doses of 600 ± 25 rads are delivered within three weeks. The nearly doubled five year survival in head andneckcancerdoesnotprovideinformation regarding the value of x. The method suggeststhatthehighoxygentensionalters the anaerobic glycolysis of Re in certain cancers. DO is unchanged. BEFORE UHF AFTER UHF 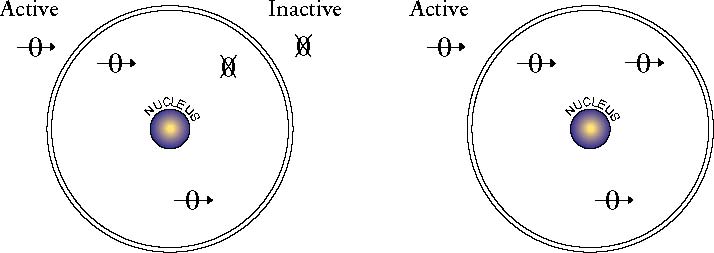 0 = EACH Re UNIT 0 = EACH Re UNIT Figure 1. 3. Conventional X-irradiation and non- electrical hyperthermia.Whole body heating to 41.8ºC (the limit of human liver tolerance) doubles the response rate to X-ray therapy. The number of targets (x) in the cell is unchanged by simple heating but there is an increase in radiosensitivity (DO value) to approximately 120 rads. 4.X-irradiationunderaerobicconditions with electrically induced hyperthermia. The effect of electrically induced heating (a maximum of approximately 41.4ºCandusuallynotabove39ºC)before X-ray therapy will increase the cell-kill by any factor between 3 and more than 100. Figure 2 (page 102) indicates such a patient. This is proof of non-thermal radio-sensitization created by 434 MHz. Even after UHF, DO, the dose required to kill 1/e cells per colony cannot be less than 90 ± 10 rads. Therefore UHF alters x to 1, irrespective of the value of x (2 to 40+) before any therapy. Very radioresistant cancers can be shown to contain at least 30 or more potentially active targets (x or Re) with an upper limit approaching 40. After UHF, . NR = NO e-D and x no longer complies with the definition “the number of targets per cell which must be killed for the cell to die.” x must be redefined as “that number which is the reciprocal of the proportion of Re units percellwhichareactivatedbyUHFbefore X-ray therapy.” 5. X-irradiation under aerobic condi-tions before and after 27 MHz, 434MHz (UHF), 915 MHz and 2450 MHzReversaloftheregime(electricalheating followedbyX-raytherapy)withalterationsin frequency of the applied electromagnetic radiation(27,434,915,and2450MHz)proves that 434 MHz has a effect different from the other three frequencies. When delivered after X-ray therapy it only enhances the x-ray sensitivitybyafactorof2whichiscommonto the heating effect of all the other frequencies. A trial of 27 MHz and 434 MHz delivered before and after X-ray therapy confirms this view for these two frequencies.4 6.HighdosageX-irradiationundertourniquet-created anaerobic conditionsLimbtumourscanbesuccessfullytreated, thusavoidingamputation,byusingatourniquet above the cancer (with the premise that thebodyproximaltothetourniquetdoesnot Figure 2. Left. Patient with a Malignant Schwannoma. 4600 rads of X-ray therapy had been delivered 2 months ago. The epilation is obvious. This treatment had no apparent effect on cancer growth rate. Right: Same patient 3 months after 11 daily doses of UHF and 150 rads X-rays. Approx. 150 times increase in radiosensitivity occured at a temperature below 41ºC. Non-electrical heating to 41.8ºC only results in a 2-fold increase in radiosensitivity, thus proving the non-thermal effect of UHF.   Figure 3. Left: A 32 year-old patient with recurrence of a fibrosarcoma of the flexor digitorum sublimus muscle. Two incomplete surgical removals and a recurrence left him with an almost useless left hand. Right: Two years later almost complete disappearance of the malignancy with preservation of normal tissue. contain cancer) to cut off the arterial blood supply to the appropriate limb whence that limb and cancer will become anaerobic after 30 minutes. Moderate heating must be applied (hot water baths, electric blanket) to prevent the limb cooling. Anoxia is the best radio protector available and limbs will tolerate six single doses of 1,600 to 1,700 rads of X-ray therapy without permanent damage.5 This proves that this dose (approximately 10,000 rads) will not kill the inactiveglutathionecyclesinthenormalcells. However the limb cancer uses only anaerobic metabolism and its glutathione cycles are thereforeactive and are killed by such doses. Calculations show that x can be at least 40 as a maximum thus establishing that cancer cells contain between 2 and 40 Re or glutathione cycles. Figure 3 (above) shows the results of such a
Table 1. Cancer doubling times measured before and after UHF radiation.method. 7. UHF irradiation after Cystine and GSSG administration434 MHz or UHF radiation will increase the mitotic growth rates of all cancers. Table 1 (above) is a list of cancers whose doubling rates were measured and these wererecordedbeforeandafterUHFradiation. In regard to the site of deposition of the energy in the cytoplasm, Re cannot be intranuclear because the nucleus does not contain oxidised glutathione (GSSG).6 The targets for UHF are the glutathione cycles Re which are in the cytoplasm. UHF energy coagulates the cytoplasm without coagulating the nucleus. UHF activates the x units from 2 or 3 up to the maximum x number per cell. This effect is most pronounced 20 minutes afterwards, but may persist for 24 to 36 hours. The dangers of all forms of electromagnetic radiations on cancer are thus due to specific absorption of the electromagnetic energy in the electrically conductive glutathione cycle–when it is active–as 2 or more Re units are always active in cancer cells. In a normal cell these glutathione cycles, Re, are only active on demand to provide the energy for the cell to divide. There are thus two methods of utilising UHF: 1) Apply UHF, make as many Re cycles as active as possible and then immediately treatthemwithadoseofionisingradiation (Figure4, page 104). The dose is optimum at approximately the resting value of DO (160 to 180 rads per day after UHF). Figure 5 (page 104) indicates some results of this approach. 2) Block the glutathione cycle by stimulating it with UHF. Figure 6 (page 105) portrays the mechanisms preventing Re from delivering energy for the cell to divide after stimulation by UHF. The disulphides cystine and oxidised glutathione, if present in very high concentration, may achieve this. Table 2 (page X Ray Therapy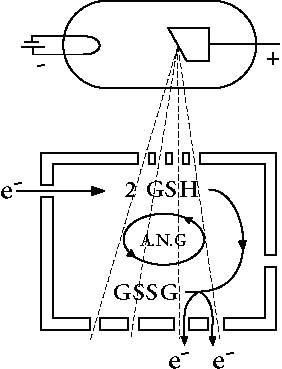 Figure4. Ionizingradiation prevents the production of electrons proceeding through normal channels to provide energy for mitosis of the cell. Ionizing (X-ray) radiation will render the insulating box–in which Re exists–conductive thus destroyingit.This explains the directaction NIL of X-ray therapy on the exponential growth system in the cell.  Figure 5. Left: Typical late stage breast cancer with massive involvement of the nodes of the axilla treated by UHF and 160 rads X-ray therapy per day to a total of 3,600 rads Right: Two years later. Complete resolution of malignancy has occured one month after treatment. The stimulating effect on normal healing is visible as the defect closed spontaneously as the cancer disappeared. The patient survived without recurrence for nearly ten years. 106) indicates the clinical progress of a division (mitosis) of each to prevent chaos. patient with bladder cancer who received Cancer can be defined as the autonomous, this treatment method. irreversible exponential growth from a single cell of a multicellular organism. Discussion A single cell of a multicellular organism Cancer becomes cancerous when its communal Evolution has produced life forms in control is lost. Single cell organisms which different cells have specific func-(bacteria, fungi, viruses) also have the tions. When two or more cells co-operate characteristics of cancer. Since each to function separately all must control the generation inherits exponential growth UHF THERAPY 434 mHZ 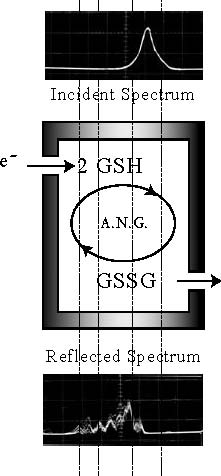 Absorbs e- e-+ GSSGReduces to 2 GSH 2e e-+Cystine Reduces to Cysteine Figure 6. The rationale for using disulphide absorption of the electrons produced when UHF stimulates Re potential then the origin of life must be a simple chemical reaction which appears to obey irreversibility and produces energy exponentially with time. Exponential GrowthWhen two molecules of GSH become one molecule of GSSG two electrons of energy are produced. Yet one electron of energy will convert one molecule of GSSG into two molecules of GSH.7 2GSH → GSSG + 2e– e– + GSSG → 2 GSH GSH + 2e– Reaction Re e– + GSSG This Cycle is effectively irreversible (either way produces energy) yet it produces energy exponentially and therefore may be the creative reaction of all life. In multicellular organisms it must be under strict control of the whole. Electrons are electricity, therefore this cycle is a dynamo and may be in some sort ofinsulatedcontainerinthemitochondrial site of the cytosol. Both GSH and GSSG are present in the cytosol of all cells except neuronornervecells(whichneverbecome cancerous). Since GSSG is not present in the nuclei, Re must be extranuclear. It may be active or dormant. All potentially active ReunitsaretheX-raytargetsxintheequation of response to X-ray therapy. The Autonomous CellThe 2 GSH →GSSG →2 GSH cycle is controlledbyevolutionaryadditionsandis inactive in adult normal cells of multicellular organisms. It is active on demand to reneweffetecellssuchasskin,blood,bowel lining–the only time this cycle in normal human cells can be electrically influenced. BLADDER CANCER J.S. Male. D.O.B. 20/3/31
Table 2. A patient who had proven cancer of the bladder stage and grading as indicated. Partial cystectomy in 1979 was followed by multiple transurethral resections (TUR). In 1983 intravenous, oral and intravesical cytotoxics were given yet the disease progressed. In 1985 a full course of X-ray therapy was given. Between February 18 and March 17 1986, 12 treatments of microwaves with the disulphides Cystine and GSSG were given which has resulted in the bladder remaining clear to date. The energy to create the extra electron in this cycle is created when d-glucose converts to l-lactic acid. Re is always active in cancer cells because the evolutionary chain of control is broken somewhere between it and its genetic control. It is a dynamo whose electrical power is used to cause cells to divide. Hence cancer is a better conductor of electricity than non-cancer and all types of radiowaves have the potential to generate electrical energy in cancer and increase its growth rate. Radiotherapy The growth rate of cancer is exponential and the mathematical expression of growth is similar to that of a rabbit population. X-rays kill exponentially and thus follow the same mathematics as that of a biological killer. For example, in the viral plague which causes myxomatosis in rabbits,the virus itself increases and infects young rabbits as their numbers increase. Similarly X-ray therapy kills exponentially 100% Years Figure7. Pilot study8a,b comparing treatment regimes: 52 successive patients were treated using a) UHF and X-rays b) hyperbaric oxygen and c) conventional X-rays. Following this series a request for a double-blind control trial was made to the Cancer Council of Western Australia and was refused in 1975. becausethex-raydamageisinheritedfrom generation to generation and acts cumulatively and because X-ray therapy directly targets the 2 GSH→GSSG→2GSH cycle (designated Re). This represents a biological control method for cancer. It is usually curative when only 2 or 3 Re units exist per cell because these are always active. It is valueless when more than 8 to 10 Re systemsexistpercellbecauseonly2or3are active and sensitive at any one time. Applying microwaves before X-ray therapy will increase the effectiveness of each x-ray dose and will automatically improve results because more Re systems are temporarily active and are simultaneously killed by the same dose of x-rays. The survival of head and neck cancer patients confirms these views8a,b (Figure 7, above). SurgerySurgery has no effect on the growth rate of any residual cancer after the operation. Surgery also cannot kill cancer exponentially. Expressed mathematically, the effectiveness of surgery is analagous to that of shooting rabbits to control them. If it were possible to shoot 100% of a rabbit population, it would cure the rabbit infestation, just as the 100% removal of neoplastic tissue cures cancer. One breeding pair of rabbits or one cancer cell prevents “cure” in either situation. The minimum prolongation of life after incompletesurgi
whereRistheresidualproportionofcancer and T2 is the cancer growth rate expressed as the doubling time in days. Cytotoxic ChemotherapyAs with surgery, cytotoxic drugs cannot kill cancer exponentially. The body has to be saturated with drugs to gain the plasma levels necessary for a cytotoxic effect. However, the toxicity of alkylating agents or antimetabolites to the host itself limits the total dose possible. These agents are toxic to all dividing cells.The behaviour of normal cells conforms to the sophisticated control mechanisms conferred by genetic information and cancer is a break in this control, permitting autonomous growth. Genetic information is thus probably irrelevant to cancer and genetic nuclear changes in cancer are causedbythe cancer and not vice versa.10 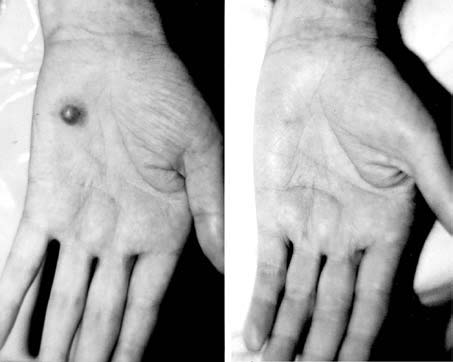 Figure 8. Kaposi’s sarcoma responds as well as any of the superficial malignacies when treated by UHF followed by low-dose X-ray therapy. Mar. 15-Apr. 2, 1993 Daily x15 Apr. 18-May. 5, 1995 Jul.14-Aug.16, 1992 2.4 gm Cystine Daily x15 Apr. 8-16, 1992 Daily x15, 1.0 gm GSSG 3.0 gm Cystine Daily x7 1gm Cystine 1.0 gm Penicillamine Disulphide 4.0 gm GSSG 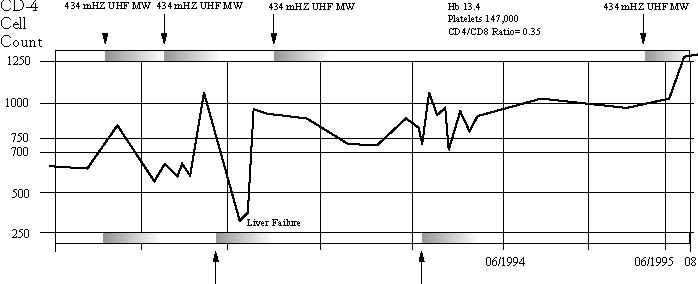 Alpha Interferon Trial Antibiotics, Steroids, P24 VLP Vaccine Trial Figure 9. Treatment time line in an HIV patient using UHF and Disulphides.Since cytotoxic chemotherapy drugs are directed at genetic (DNA/RNA targets) this method is the equivalent of poisoning the rabbits’ burrows after the rabbits have run away. Residual poison in ecological systems indiscriminantly injures other life forms besides the intended target. This is equivalent to the injury sustained by the host’s immune system, and impedes or prevents normal recovery. HIV TreatmentHIV infection spreads exponentially in a susceptible population and therefore must have the same energy source as life and cancer. It is thus rational to treat it by the same routine used for cancer. Figure 8 (above) shows the response of Kaposi’s sarcoma to eight daily doses of UHF each followed by 180 rads of X-ray therapy (total dose of 1440 rads). The responses with and without UHF are identical to skin cancers generally. Figure9 (page108)showsatreatment timeline of a young man, HIV positive, who was treated identically to cancer and shows that this hypothesis is correct. Seven hundred CD4 cells are considered to be the lower limit of normal. This patient presented with 650 T4 cells and starting on an alpha-interferon combined with microwaves. This had no apparent effect on the disease. He was re-treated in August of 1992 with cystine and GSSG along with microwaves and some delayed improvement in T4 count resulted. A final treatment in April to May 1995 used higher doses of disulphides and boosted the patient’s T4 count considerably. For the four months since his last treatment he has had a normal T4 cell count (1250 ±100) and a T8 cell count whichisapproachingnormalwithaT4/T8 ratio greater than 1. He is completely well without any secondary infections and has returned to his pre-HIV infection weight andphysicalcharacteristics.Itthusappears that a simple, non-toxic, safe method of controlling HIV has been discovered. Summary1.The energy source for life and cancer is created by anaerobic glycolysis interchanging oxidised and reduced glutathione, a system denoted Re. All cells except neurons have two or more of these systems. In cancer only two or three are active at any one time. Re is situated in the extra nuclear components of the cell. 2. X-ray therapy directly targets Re. 160 rads will kill an active system, but 10,000 rads may not destroy an inactive one. Doses well in excess of 1650 rads daily for six doses in vivo are required to kill an inactive Re. 3.UHF will activate all or most of the potentially active Re systems in the cell for approximately 20 minutes. Therefore UHF must be given before X-ray therapy if its radiosensitizing effects are going to be optimised.
References
Biology. ed. W E Pryer. New York. Academic Press.1976; 2: 67-71. 8a. Nelson A J M & Holt J A G: Combined MicrowaveTherapy. MedicalJournalofAustralia. 1978; 2: 88-90. b. Nelson A J M & Holt J A G: Combined MicrowaveTherapy. MedicalJournalofAustralia. 1985; 13: 707-708. 9. Shidnia H et al: Clinical Experience with HyperthermiainConjunctionwithRadiation Therapy. Oncology, 1993; 50: 353-361. 10.Holt J A G.The Glutathione Cycle is the Creative Reaction of Life and Cancer. Cancer CausesOncogenesandNotViceVersa. Medi-cal Hypotheses. 1993; 40: 262-266. 11. Baker Z: Glutathione and the Pasteur Reaction. The Biochemical Journal, 1937; 31: 980-986. | |||

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)